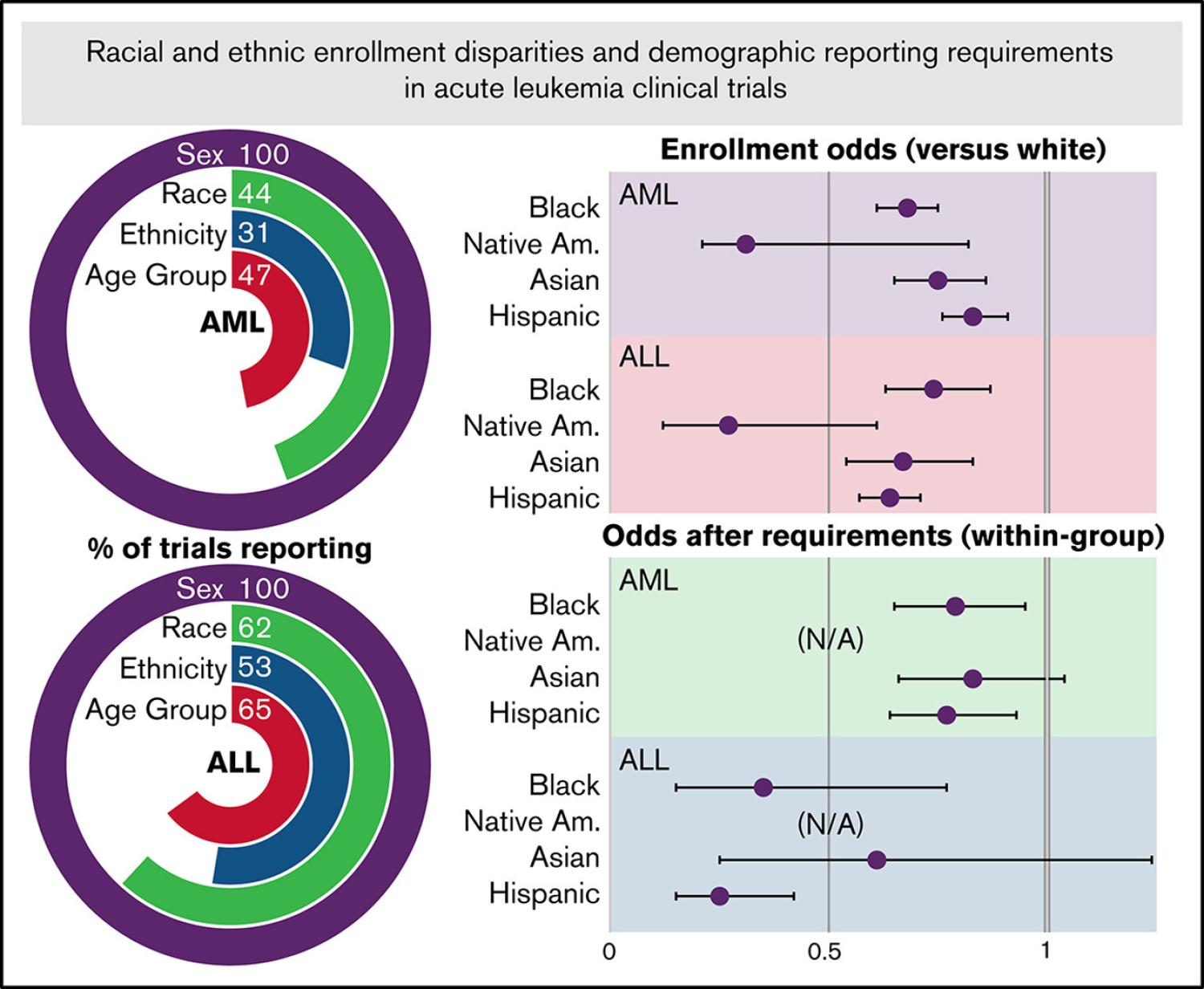
Data regarding racial and ethnic enrollment diversity for acute myeloid leukemia (AML) and acute lymphoid leukemia (ALL) clinical trials in the United States are limited, and little is known about the effect of federal reporting requirements instituted in the late 2000s. We examined demographic data reporting and enrollment diversity for ALL and AML trials in the United States from 2002 to 2017, as well as changes in reporting and diversity after reporting requirements were instituted. Of 223 AML trials and 97 ALL trials with results on ClinicalTrials.gov, 68 (30.5%) and 51 (52.6%) reported enrollment by both race and ethnicity. Among trials that reported race and ethnicity (AML, n 5 6554; ALL, n 5 4149), non-Hispanic (NH)-Black, NH-Native American, NH-Asian, and Hispanic patients had significantly lower enrollment compared with NH-White patients after adjusting for race-ethnic disease incidence (AML odds ratio, 0.68, 0.31, 0.75, and 0. 83, respectively; ALL odds ratio, 0.74, 0.27, 0.67, and 0.64; all, P # .01). The proportion of trials reporting race increased significantly after implementation of the reporting requirements (44.2% to 60.2%; P 5 .02), but race-ethnicity reporting did not (34.8% to 38.6%; P 5 .57). Reporting proportions according to number of patients enrolled increased significantly after the reporting requirements were instituted (race, 51.7% to 72.7%; race-ethnicity, 39.5% to 45.4%; both, P, .001), and relative enrollment of NH-Black and Hispanic patients decreased (AML odds ratio, 0.79 and 0. 77; ALL odds ratio, 0.35 and 0.25; both P # .01). These data suggest that demographic enrollment reporting for acute leukemia trials is suboptimal, changes in diversity after the reporting requirements may be due to additional enrollment disparities that were previously unreported, and enrollment diversification strategies specific to acute leukemia care delivery are needed.
Special collection
Category